The only events I can seem to attend these days are Health Extension Salons. But I also attended the 2013 Quantified Self Conference in San Francisco, so I was exposed to plenty of new ideas there as well, which I will be sharing soon. Health Extension Salon #13 was held at Runway SF, which is a cross between a co-working space and an incubator. At the beginning of the talks, the operations person from Runway said that their uniquely high percentage of shared public space supercharged the startups based there as the teams intermingled and ideas were cross-pollinated. Apparently they have have a good number of successful exits, which for an incubator must mean getting funding or something. It’s an amazing space, but they are still pretty stealthy. They don’t even have a website that I could locate.
For those who don’t know:
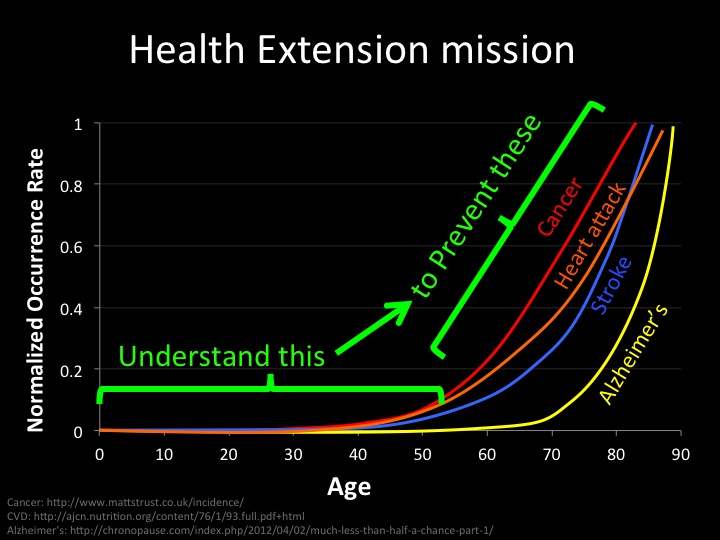
The Health Extension community is committed to collaborative action to extend healthy and happy human life spans to 123 years and beyond. Our members are scientists, entrepreneurs, and social influencers dedicated to fixing the degenerative cellular processes that cause deadly human diseases.
Health Extension was founded and is executively directed by scientist/entrepreneur Joe Betts-LaCroix. Joe gave his standard presentation pointing out how absurdly underfunded aging related research is. Basic research into the biochemical processes behind aging represent a tiny fraction of healthcare spending, while aging related diseases account for the vast majority of healthcare costs. So obviously there is a disconnect somewhere.
The field of aging research it clearly underfunded, so Google’s new Calico project seems very encouraging. Aubrey De Grey is certainly in favor of it. Google clearly has cash to throw at the problem, but some folks question whether they can find the right talent. However, accomplished biotech scientists have assured me that Calico’s CEO Arthur Levinson has an extraordinary contact list and can get the talent he wants. So the hunt is on in earnest with the data wizards over at Google on the case.
Joe highlighted some very interesting findings by researchers at the University of Pittsburgh School of Medicine. They looked at lymph nodes and reconsidered why cancers often begin their deadly migration of metastasis there. Lymph nodes provide direct access to nutrients, growth factors, and signaling proteins that aid in cell recruitment. Then they turned this idea on its head and asked – “Hey, why don’t we see if we can grow little mini-organs there in the lymph nodes?” And so they did. They injected mouse lymph nodes with liver cells, and the little masses of liver cells that grew in the lymph nodes were functional enough to save the mouse from liver failure. Then they performed the same trick with thymus cells and pancreatic cells. So yeah, that sort of blew my mind.
When you stop to think about it, you can imagine ways to make all organs fault tolerant by overloading lymph nodes with little micro-organs distributed throughout the body. This almost reminds me of highly-available computer clusters. Of course, evolution probably arrived at a centralized liver for a reason. It may be that a single large mass of liver tissue can more quickly transfer bigger doses of important factors like glycogen to other vital organs. Messing with any complex system like this will surely lead to a bunch of broken functions. But if I were faced with the choice of that or liver failure, I might take the chance. There aren’t enough donor livers to go around.
Next, Joe went on to relate that HE’s Aging Variant Database Project was rejected by the Nucleic Acid Research journal. Apparently an editor fell victim to the halo effect bias. They decided that the database must be tainted because it was hosted on a site that also hosted links to life extension topics and the mere mention of life extension is disreputable. This database is a meta-analysis of existing studies meant to identify genetic variants related to aging. This certainly isn’t quackery or pseudo-science and most of the reviewers realized that. But Nucleic Acid Research is a prestigious journal. And prestige is something that must be jealously guarded. So the Health Extension researchers will be submitting the Aging Variant Database to another journal, possibly the modern, open-source PLOS One.
One thing I like about Health Extension is all the interesting people you can meet during the social periods. I bumped into biotech entrepreneur and fellow Oaklander Ryan Bethencourt, who co-founded Sudo Room, Counter Culture Labs, and BerkeleyBiolabs. He told me a bit about this “hackubator” Berkley Biolabs is setting up, which is biotech space for scientists with promising ideas to work out proofs of concept. I guess there is this new crowdfunding site, Wefunder.com, that will be involved somehow. He then introduced me to Andre Watson, who won my admiration first by having seen every Star Trek episode, and secondly by telling me a bit about his work on nanotechnology for genome editing. At Foresight this year, I had heard George Church mention the CRISPR gene editing technique that is a biomimicry of a bacterial proto-immune system. So accurate human gene editing therapies might be coming down the pipe at some point.
As much I do love Star Trek (Picard not Kirk), I have this dark side that is contrary to the Gene Roddenberry optimism of Star Trek. I am picturing governments editing the genes of their citizenry to make them more pliable. Imagine the marketing potential there! I asked Andre if he thought gene editing would be used for good or evil, and he sensibly replied “both.” Which is, of course, the fate of all technology. But a world where genes can be altered at will or against your will is very strange to imagine. Will genetic traits be taken up and discarded like fashion statements? Will we accidentally break all manner of delicately balanced genetic network interactions and wreak untold havoc? It’s hard to say.
I then went on to talk to another scientist that I admire, JR, to hear what he was up to. I had been wondering why SENS didn’t seem to be pursuing a strategy to activate protective pathways that prevent aging, similar to what Cynthia Kenyon found in her long-lived nematode mutants. JR pointed out that since calorie restriction doesn’t even seem to increase longevity in mice, let alone primates, it would be difficult to exploit those pathways that Kenyon discovered. He framed the question thus: would it be easier to tweak metabolism to prevent damage or to repair damage once it occurred? He considered the latter to be simpler. And this seems consistent with the SENS approach. Repair damage as it occurs. And that is perfectly reasonable, but I find myself a bit disappointed. Kenyon seemed to point toward hidden capabilities just waiting to be unlocked. Like a biological equivalent of the software Easter egg. But practical people are pointing to something more like automobile maintenance. Not that I would turn down longevity via that method. I just want to believe I can fly.
Err, yeah. So then JR clued me into the immense potential of bone marrow transplants. These have been found to “cure” AIDS. It’s not clear how this applies to his own work, but he does like to work with blood because it’s easier to manipulate than organs or solid tissues. See, this is why I like JR so much. His approach appeals to my pragmatic side. I look forward to seeing what practical human rejuvenation techniques he will develop.
Again, this is why I love Health Extension Salons. I have already been inundated with exciting ideas and the main speaker hasn’t even presented yet. The main speaker was Sean Mooney, Director of Bioinformatics at the Buck Institute for Research on Aging. He started out by encouraging biotech startups to consider government SBIR and STTR grants to access non-dilutive capital. He, like many academics, sits on various “study sections” that review these grants and said that he often doesn’t see enough projects worth funding. I had never heard of these study sections, but I guess the recent government shutdown really threw a wrench into the works and some think that this threatens the US position as the worldwide leader in scientific research. Of course my libertarian friends would have something to say in rebuttal, I’m sure.
Mooney then asked the room how many people had their entire genome sequenced. I initially raised my hand, foolishly thinking that my paltry 23andMe SNPs qualified. But Mooney repeated the phrase “entire genome.” And only one person raised their hand. Apparently they had participated in a study through Personalis. Mooney was impressed and said that he had asked that question at many conferences but rarely had anyone raise their hand. He predicted that the entire genome sequencing would become very common as soon as the price plummets. And the price is plummeting exponentially in a way that would warm Ray Kurtzweil’s heart.
<insert logarithmic graph here>
Mooney talked a bit about his work in translational research, which aims to bridge the gap between basic and applied research to move findings from research labs into medical clinics and move empirical data from the clinics back into the research labs. This is a fascinating topic that certainly warrants further examination, but then Mooney went on to an even more interesting topic. He brought up the CAGI challenge, which invited researchers to predict clinical medical outcomes based on genomic data using George Church’s Personal Genomes Project. Currently, 23andMe gives you some estimates of that sort of thing for many diseases, but apparently their stuff doesn’t cut the mustard in the clinical world. So this was a pretty tough challenge and actually none of the teams were able to accurately match more than a small minority of the genomes to medical outcomes. I found this surprising. I would have expected better results. It’s not clear if this poor showing was the result of insufficient data, or if nurture really does trump nature in medical outcomes. I understand that throwing methylation information into the mix would help improve the predictive power. One biologist I related these finding to quipped that he wasn’t surprised by the results since DNA can’t tell you whether a person is alive or dead.
So what does this mean? It seems to mean that scientists don’t yet have good models to predict what the real effect of genes are on phenotypes. Yeah, so what good is this genetic data then? Best take those 23andMe predictions with a grain of salt. Mooney was quick to point out that he obviously wasn’t bearish on genomics being a bioinformatics person. While genetic data might not be ready for clinical prime time, he had little doubt that doctors will be using genetic data in the near future.
One challenge to reaching this goal is that gene expression differs from tissue to tissue. It was speculated during discussion after the talk that these differences in gene expression could pose unforeseen risks to Induced Pluripotent Stem Cell treatments. Consider a cheek cell which expressed a mutation that increased the chance of liver disease. This would be harmless since the cheek cell isn’t in the liver, but if that cell were scraped and converted into a stem cell to regrow liver tissue… well, that would be a problem. At first, I naively thought that IPS stem cells would be better for medicine since the immune system wouldn’t need to be suppressed to avoid rejection. But several scientists I spoke with pointed out that the complexity of modifying IPS posed more risks than naturally pluripotent embryonic stem cells, though having your own cord blood would be optimal. Anyone have parents forward thinking enough to bank that stuff? No? Too bad.
Health Extension continues to provide an amazing forum to learn about real science from serious scientists who are pushing the field of aging research forward. The more I learn about this stuff, the more daunting the problems seem sometimes. But there are other ideas that seem so much closer to implementation, such as Justin Rebo’s blood scrubber, or even the idea of blood infusions from young to old to provide regeneration. Health Extension is a real thing that can happen if the right resources are focused upon it, and that’s an exciting future to consider.